





One Policy Does Not Fit All
Maryland Governor Larry Hogan has won praise for his cautious, conscientious, and steady leadership during the COVID-19 pandemic. The steps he and local leaders have taken certainly mitigated a public health catastrophe and saved lives. Nothing in what follows should be taken as hindsight-inspired criticism of those steps, nor as a call for a radical change of course based on disregard of the real danger this virus poses.
Now, as the state and nation move forward, policy-makers must walk a tightrope. Lean too far in the direction of minimizing risk to public health and we get further devastation of the economy (which will itself have adverse health effects); restart the economy prematurely and progress against COVID-19 may be squandered. The modest goal of this piece is to review some facts that may help us walk that tightrope along with Maryland officials and understand some of the principles that will surely guide the gradual, phased re-opening process recently described by the Governor.
Some, of course, are appalled at the idea of re-opening anytime soon; their mantra is that we should stay locked down “as long as one life might be saved.” Others think the lockdown is unnecessary and we needed to get back to work yesterday. Each group views the other with suspicion if not anger.
Both sides need to moderate their views. Note first: we never maximize either safety or economic output, but rather try to optimize our pursuit of both. For example, we use cars despite their risks (nationally, about 100 fatalities per day in normal times) because the benefits of doing so far outweigh the costs – but we also have speed limits, drunk driving laws, guardrails, and more to mitigate these risks. We should similarly factor the benefits of a functioning economy – including the mental and physical health benefits thereof – into our views about the lockdown. And we should weigh the risks of ending it with due regard for the fact that COVID is not “just the flu” – especially for some groups.
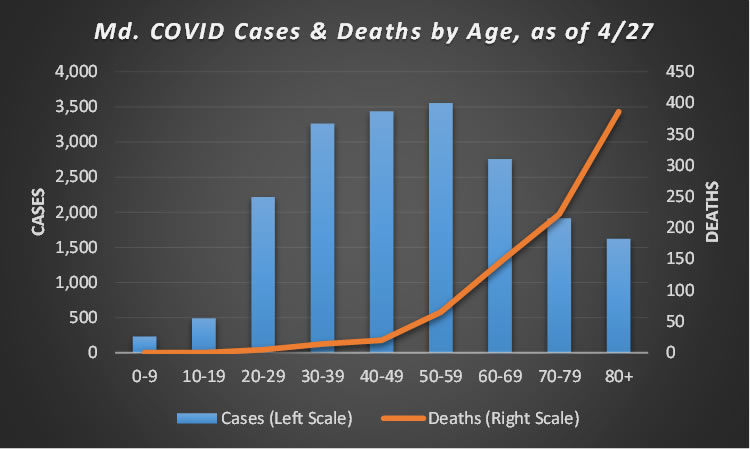
That is one of the most widely-noted aspects of this pandemic: it is having a disparate adverse impact on the elderly and those with prior health conditions. As the graphic above shows, this is especially true in Maryland, where (as of 4/27) 41% of COVID fatalities have involved patients over 80 years of age – while that group accounts for only 8% of confirmed cases and 4% of the state’s population. By contrast, just 3.6% of Maryland’s COVID fatalities (counting both confirmed and suspected cases) have been to those under age 50, a cohort that accounts for 49% of confirmed cases and 65% of the state’s population. To date, there have been zero fatalities among Marylanders under age 20, and only five among those aged 20-29.
There’s also considerable geographic variation in both case counts and fatalities, as the graphic below shows. As this is written, four lightly-populated Maryland counties (Caroline, Garrett, Somerset, and Worcester) have yet to record a COVID-related fatality; 15 of the state’s 24 jurisdictions have less than ten fatalities per 100,000 residents. On the other hand, a half-dozen counties, all well-populated with the exception of Kent, have experienced 20 or more fatalities per 100,000 residents.
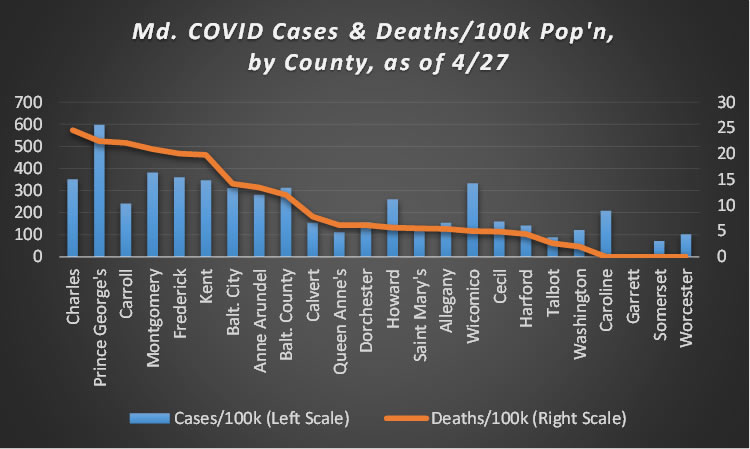
The data on case counts are a little sketchy, since they’re sensitive to testing frequency, but there’s a lot of geographic diversity there, as well. With some notable exceptions, denser and more highly-populated areas seem to have higher case counts than low-density and/or low-population areas.
Finally, though there is less data documenting this fact, it is quite clear that the “collateral damage” of the lockdown varies greatly by class. If you are high-education and high-income, it is quite likely that you are able to maintain your standard of living, work from home, and even keep your kids up to speed with online learning technology. If you are a single mom who has been working paycheck-to-paycheck waiting tables, your experience of this lockdown is wildly different.
The bottom line is that up to now, state policy on COVID has been “one size fits all.” With the exception of classifying certain businesses as essential and others non-essential, we have imposed school closures, stay-at-home orders, and other restrictions without many distinctions as to people or places.
Going forward, that is likely – and, in fact, is necessary and desirable – to change. The instant it appears likely that we have “flattened the curve” on hospitalizations, created enough capacity to deal with fluctuations in case counts, and have the capability (via more efficient testing) to identify possible “spreaders” and limit their impact, we must see a more tailored, customized policy on COVID.
That would mean some low-population-density, low-risk counties get to do some things (e.g., shop or dine – at a distance) that others do not, and do them sooner. It may mean that elementary school students (for whom Zoom lectures and online exercises are ill-suited) return to classes before high school or college students – but that individual students living in households with elderly family members may have to continue under stay-at-home orders. And it almost certainly means that if you are older, or have a compromised health profile, you will face more severe quarantine restrictions longer – and that financial relief packages should be targeted to accommodate such restrictions.
None of this will seem fair, and some of it will seem frightening. To get to the other end of the tightrope successfully, however, it’s essential.
Stephen J.K. Walters (email: swalters@mdpolicy.org; Twitter: @SJKWalters) is chief economist at the Maryland Public Policy Institute and the author of Boom Towns: Restoring the Urban American Dream.